
groups » Informed Consent and Community Engagement » Informed Consent and Illiterate Participants - how do you explain problematic concepts?
Dear all
There have been many discussions on the Global Health Network, and in global health research in general, about informed consent and illiterate participants.
We're interested in how you discuss a study with participants who might not understand the core concepts. For example, how do you explain randomisation? And how do you explain what a vaccine will do, or the concept of an intervention that is just being tested?
We've heard that some members have used illustrations to explain the different concepts: for example using a picture of the lottery to explain randomisation. It would be really interesting to hear/see examples of illustrations your site have used. How did you go about developing and testing these?
What other things to you do at your sites to explain these concepts?
We look forward to hearing from you!
The Editorial Team
-
 Henok Negussie
8 May 2013
Henok Negussie
8 May 2013
I work in a randomized controlled trial of podoconiosis treatment in northern Ethiopia. I would like to comment on the process of obtaining informed consent and explaining some concepts such as randomization.
Based on experiences gained from a genetic study in western Ethiopia (Tekola et al, 2009), we plan to use an innovative approach - Rapid Ethical Assessment (REA) - to guide the consent process and make it appropriate to the study setting prior to initiation of the main trial. In the REA we make use of qualitative research techniques (FGDs and IDIs) with religious and local community leaders and community members, to gain an understanding of how best to approach the community and individuals, how to disseminate information about the study and how to obtain informed consent for participation in ways preferred by the community. Accordingly, the format of information sheets and consent forms as well as sensitization will depend on responses given by participants in the REA. Thus, concepts such as randomization will be explored in the REA and the best descriptions be used later in the trial. Articles on REA are available from www.plosntds.org and http://www.biomedcentral.com/1472-6939/10/13 . For more information on podoconiosis please visit www.podo.org.
I hope this helps. -
TAFFA ISSAH
3 May 2013
INFORMED CONSENT;A PROCESS BY WHICH A FULLY INFORMED PERSON PARTICIPATE IN CHOICES ABOUT HERSELF/HIMSELF.
The Health Demographic Surveillance System (HDSS) is a population registration system that monitors health and demographic dynamics in a geographically defined population.
The HDSS provides a platform to test and evaluate public health interventions such as vaccines and provides a suitable sampling frame for epidemiological studies. -
 The Editorial Team
3 May 2013
The Editorial Team
3 May 2013
Thank you, Suzanna, Augustine and Omari for sharing your views. Suzanna, the documents you attached are brilliant and really inspiring. If others have developed similar documents it would be fantastic to see examples?
In the meanwhile I came across this article and thought it might be of interest for this discussion - it's about comprehensibility of ICFs: mhttp://clinicaltrials.ploshubs.org/article/info:doi/10.1371/journal.pone.0047023
-
S McDonald
24 Apr 2013
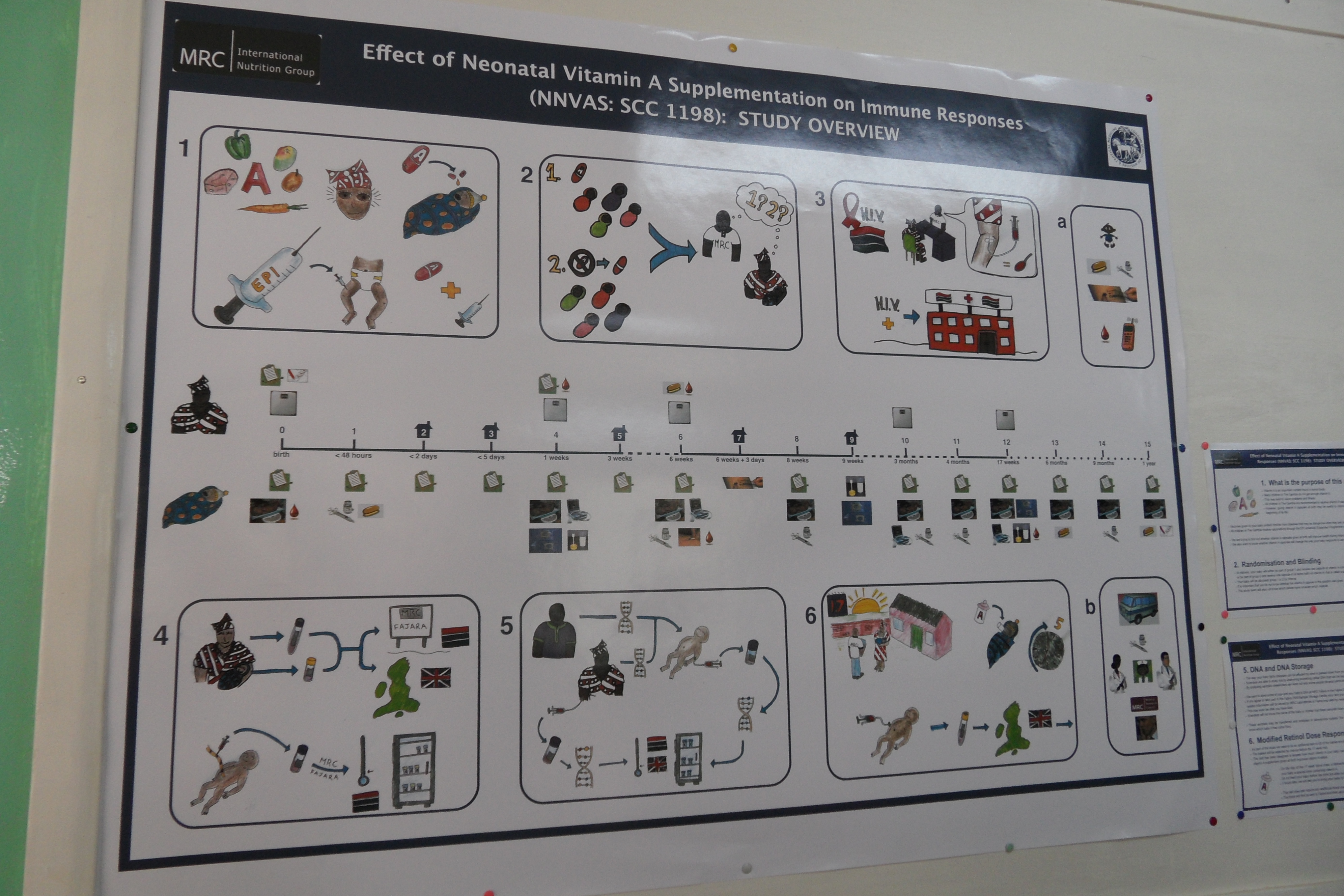
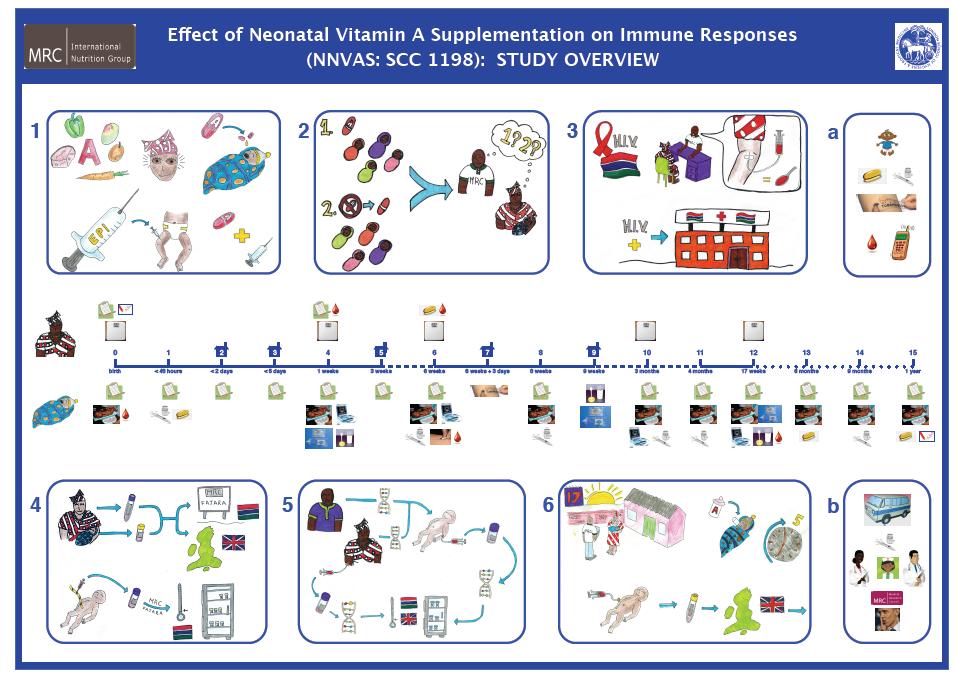
I work with the MRC in the Gambia, and would like to share the experience of a nutrition trial, funded by WHO, via the Bill and Melinda Gates Foundation.
We developed the attached poster as we were recruiting women who had just given birth and its wasn’t possible to really sensitize them earlier than at the labour ward. Culturally in The Gambia it is very taboo to discuss pregnancy and unborn babies and so it is quite challenging to sensitize during the antenatal period. Therefore this poster was displayed in the Govt. antenatal clinic so that the mothers attending the clinic at least knew that there was an MRC study running that was recruiting babies. We weren’t expecting the government midwives to necessarily have the time to explain the poster, but each numbered figure in the poster had accompanying text paragraph (bullet points) displayed next to the poster.
Recruiting at birth was a much bigger issue with our European based ethics boards, but the local ethics board had a much greater understanding that the birthing process is not viewed the same here as in most developed countries. It really isn’t unusual for mums to be up and out of the centre within an hour of giving birth and back to looking after all their other children and other domestic duties etc.
It was a complex trial in terms of the numbers of study visits and how quickly after birth the visits happened. Between birth and one week of life the baby was on its 5th study visit!! Therefore I wanted to try and make it as clear as possible for the mothers what the trial was about. Secondly as a way to help them discuss it with their family who may also most likely be illiterate, as in The Gambia the consent of other older and male family members is very important.
We broke the whole of the ICF down into the 6 main explanatory figures, with rights and benefits and the study timeline described separately. The top of the timeline was what happened to mum at each visit and the bottom was everything that happened to the baby.
Some of the issues were really difficult to explain: ‘DNA will be stored in the biobank’, and ‘samples will be sent overseas for testing’ – we weren’t really expecting the mums to necessarily grasp the concept of DNA which is what we’ve drawn in the poster. This was described as ‘hertiability’ and ‘characteristics inherited from your mum and dad’ etc in the written ICF document.
The poster was also displayed in the MRC clinic. This was used as a tool by the nurses/FWs at each clinic visit to explain how far through the study the mum and baby were and what was going to happen at that visit. If the mums had questioned they used the poster to help explain things.
Suzanna McDonald and Tom Holliday (2011), MRC International Nutrition Group
Attached files: SAM_2608.JPG, gambia_psoter.jpg -
Omari Kimbute
23 Apr 2013
I will comment on the issue of placebo.The previous community based clinical trial I worked on involved a use of placebo and I would like to share my experience with you all.
It was not simple issue to introduce placebo not only to participating communities but also to leaders and government officials even for those working in the medical field.
The approach of the study was to introduce the study to the district authorities before going to the community and I remember that some of the leaders suggested that we should not mention about placebo otherwise we will not be able to get study subjects.
The approach we used was to use a consent form as our guide as it included everything and at the end of the talk we could invite questions and if the question of placebo was not asked we tabled it for discussion.
We were able to deal with the issue of placebo by first of all to talk about research and benefits of research to the communities.
In this study there was a 50% chance of getting a capsule with an active ingredient and the cases we were looking for were those who can not be treated at home(for sure they were on their way to a nearest unit of treatment) and the point taking a 50% chance of having medicine with and active ingredient was well accepted.
In summary people should be told why they are asked to participate in the research,benefit/risk issues and discuss everything in detail (including placebo) then they can be in position to make up their minds. -
 AUGUSTINE ONYEAGHALA - Senior Contributor
22 Apr 2013
AUGUSTINE ONYEAGHALA - Senior Contributor
22 Apr 2013
No doubt, informed consent process has always been the bane of unethical clinical research. The reasons are numerous ,one of which is illiteracy. Nonetheless, modern administration of informed consent and the explanation of the entire research process including randomization has applied the use of multi media with lots of graphics. This has been proved to be very efficient among the illiterate population.
One other thing that works well is the entire explanation of the randomization process using the local language that the participant understands. Hope this helps?
{kind=link}
{kind=link}
Please Sign in (or Register) to view further.